
Search
- Page Path
- HOME > Search
Review Articles
- Diabetes, obesity and metabolism
- Glucagon-Like Peptide-1 Based Therapies: A New Horizon in Obesity Management
- Jang Won Son, Soo Lim
- Endocrinol Metab. 2024;39(2):206-221. Published online April 16, 2024
- DOI: https://doi.org/10.3803/EnM.2024.1940
- 1,348 View
- 101 Download
-
 Abstract
Abstract
 PDF
PDF PubReader
PubReader  ePub
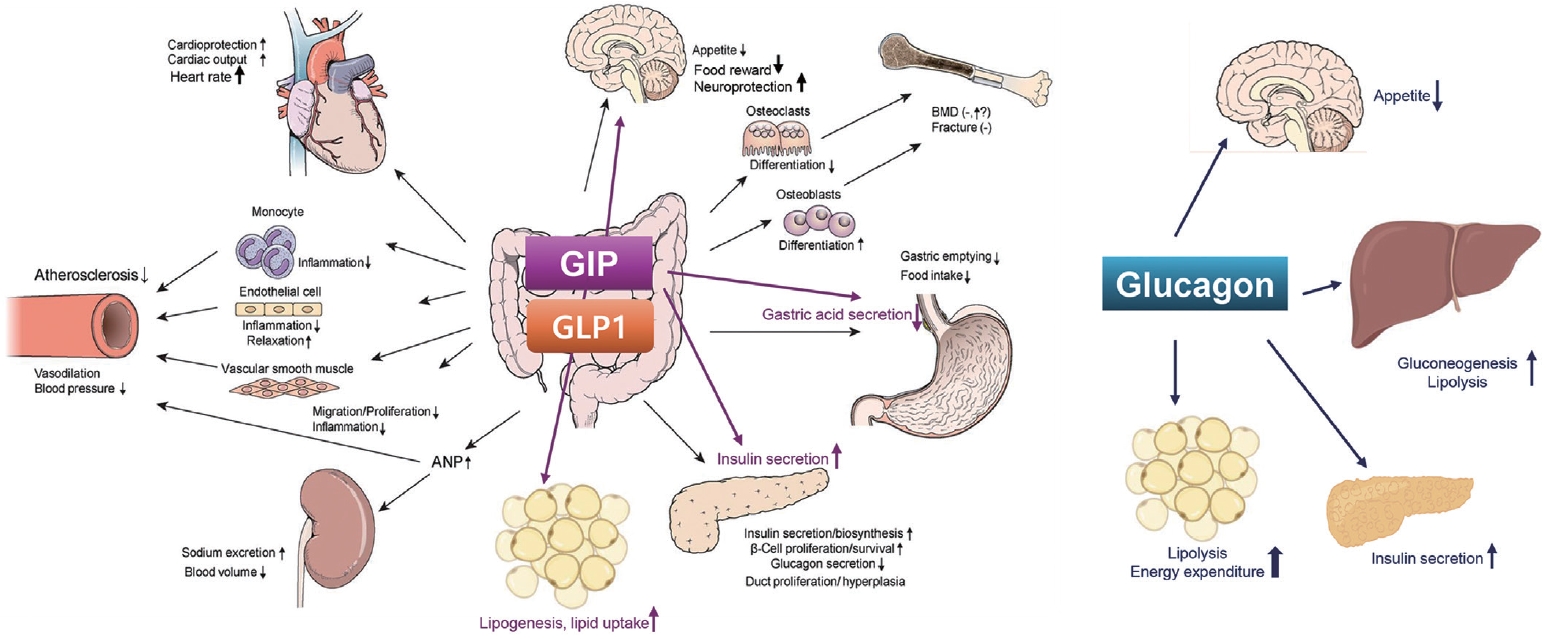
ePub - Obesity is a significant risk factor for health issues like type 2 diabetes and cardiovascular disease. It often proves resistant to traditional lifestyle interventions, prompting a need for more precise therapeutic strategies. This has led to a focus on signaling pathways and neuroendocrine mechanisms to develop targeted obesity treatments. Recent developments in obesity management have been revolutionized by introducing novel glucagon-like peptide-1 (GLP-1) based drugs, such as semaglutide and tirzepatide. These drugs are part of an emerging class of nutrient-stimulated hormone-based therapeutics, acting as incretin mimetics to target G-protein–coupled receptors like GLP-1, glucose-dependent insulinotropic polypeptide (GIP), and glucagon. These receptors are vital in regulating body fat and energy balance. The development of multiagonists, including GLP-1–glucagon and GIP–GLP-1–glucagon receptor agonists, especially with the potential for glucagon receptor activation, marks a significant advancement in the field. This review covers the development and clinical efficacy of various GLP-1-based therapeutics, exploring the challenges and future directions in obesity management.

- Diabetes, Obesity and Metabolism
- Human Tissue-Engineered Skeletal Muscle: A Tool for Metabolic Research
- Ji-Hoon Kim, Seung-Min Yu, Jang Won Son
- Endocrinol Metab. 2022;37(3):408-414. Published online June 29, 2022
- DOI: https://doi.org/10.3803/EnM.2022.302
- 4,069 View
- 164 Download
- 1 Web of Science
- 2 Crossref
-
Abstract
PDFPubReader ePub
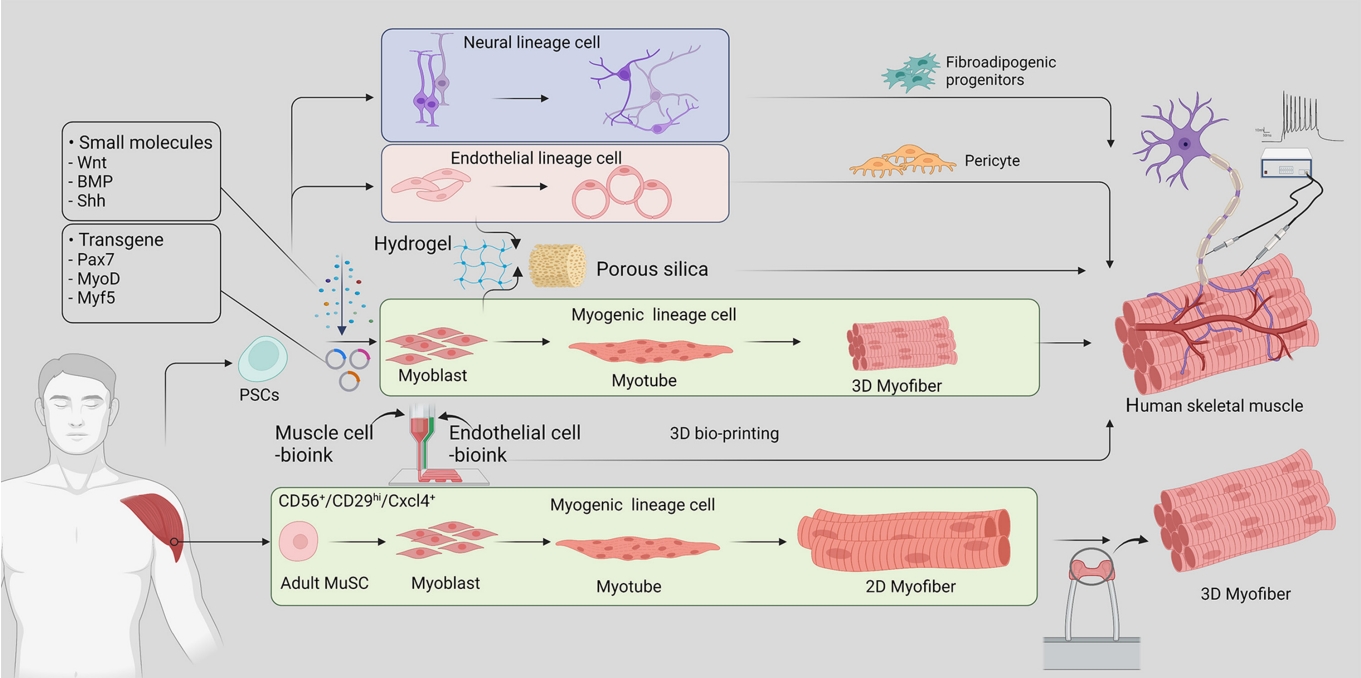
- Skeletal muscle is now regarded as an endocrine organ based on its secretion of myokines and exerkines, which, in response to metabolic stimuli, regulate the crosstalk between the skeletal muscle and other metabolic organs in terms of systemic energy homeostasis. This conceptual basis of skeletal muscle as a metabolically active organ has provided insights into the potential role of physical inactivity and conditions altering muscle quality and quantity in the development of multiple metabolic disorders, including insulin resistance, obesity, and diabetes. Therefore, it is important to understand human muscle physiology more deeply in relation to the pathophysiology of metabolic diseases. Since monolayer cell lines or animal models used in conventional research differ from the pathophysiological features of the human body, there is increasing need for more physiologically relevant in vitro models of human skeletal muscle. Here, we introduce recent studies on in vitro models of human skeletal muscle generated from adult myogenic progenitors or pluripotent stem cells and summarize recent progress in the development of three-dimensional (3D) bioartificial muscle, which mimics the physiological complexity of native skeletal muscle tissue in terms of maturation and functionality. We then discuss the future of skeletal muscle 3D-organoid culture technology in the field of metabolic research for studying pathological mechanisms and developing personalized therapeutic strategies.
-
Citations
Citations to this article as recorded by
- Human‐based new approach methodologies to accelerate advances in nutrition research
Manuela Cassotta, Danila Cianciosi, Maria Elexpuru‐Zabaleta, Inaki Elio Pascual, Sandra Sumalla Cano, Francesca Giampieri, Maurizio Battino
Food Frontiers.2024;[Epub] CrossRef - Key indicators of beef safety and quality as important aspects of conservation
S. V. Furman, I. M. Sokulskyi, D. V. Lisohurska, O. V. Lisohurska, B. V. Gutyj
Ukrainian Journal of Veterinary and Agricultural Sciences.2024; 7(1): 68. CrossRef
- Human‐based new approach methodologies to accelerate advances in nutrition research
Editorial
- Diabetes
- Unlocking the Therapeutic Potential of Glucagon-Like Peptide-1 Analogue and Fibroblast Growth Factor 21 Combination for the Pathogenesis of Atherosclerosis in Type 2 Diabetes
- Jang Won Son
- Endocrinol Metab. 2021;36(1):57-59. Published online February 24, 2021
- DOI: https://doi.org/10.3803/EnM.2021.109
- 3,008 View
- 117 Download
Review Article
- Miscellaneous
- Systems Biology: A Multi-Omics Integration Approach to Metabolism and the Microbiome
- Jang Won Son, Saeed Shoaie, Sunjae Lee
- Endocrinol Metab. 2020;35(3):507-514. Published online September 22, 2020
- DOI: https://doi.org/10.3803/EnM.2020.303
- 6,616 View
- 290 Download
- 7 Web of Science
- 6 Crossref
-
Abstract
PDFPubReader ePub
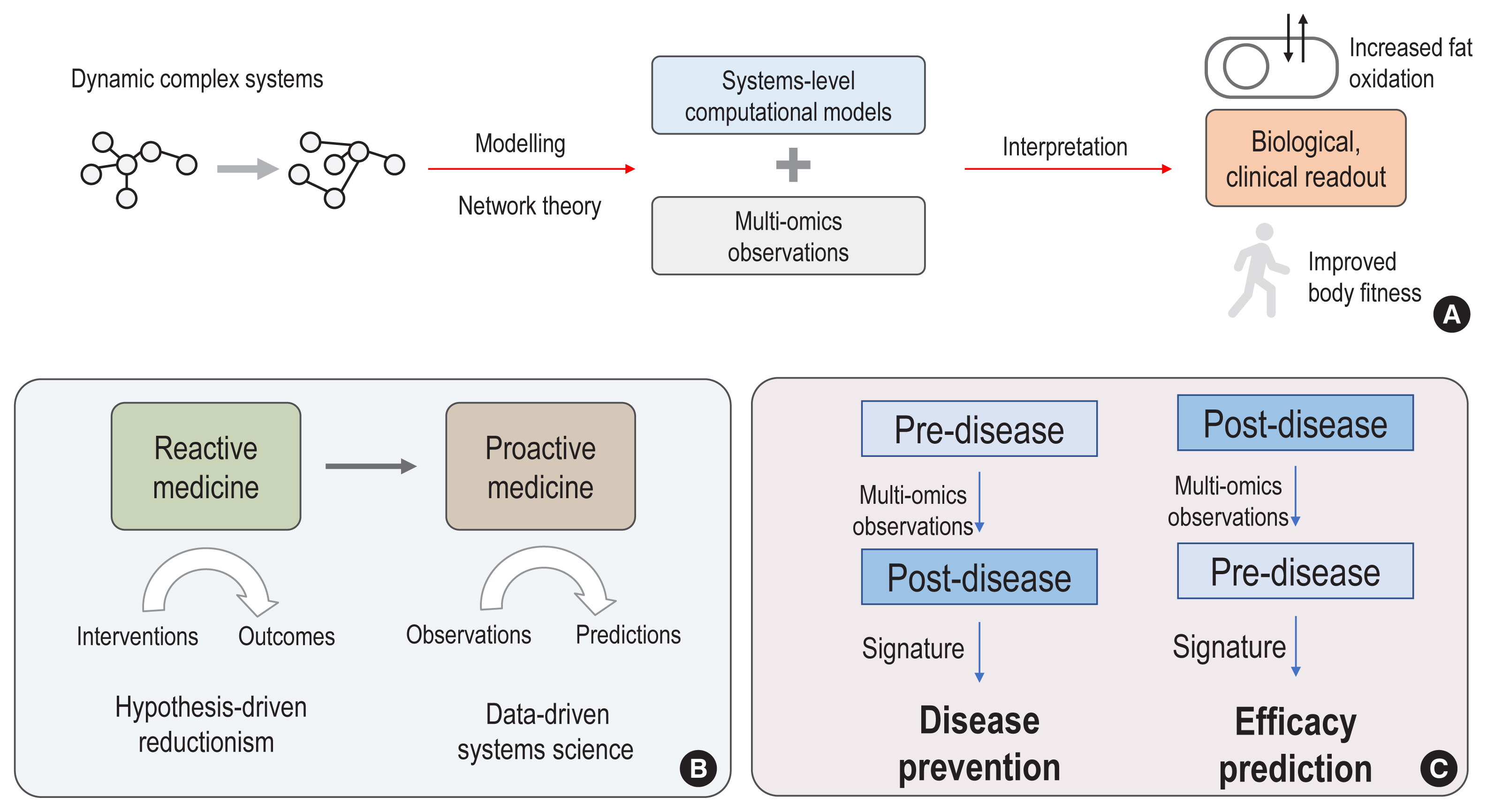
- The complex and dynamic nature of human physiology, as exemplified by metabolism, has often been overlooked due to the lack of quantitative and systems approaches. Recently, systems biology approaches have pushed the boundaries of our current understanding of complex biochemical, physiological, and environmental interactions, enabling proactive medicine in the near future. From this perspective, we review how state-of-the-art computational modelling of human metabolism, i.e., genome-scale metabolic modelling, could be used to identify the metabolic footprints of diseases, to guide the design of personalized treatments, and to estimate the microbiome contributions to host metabolism. These state-of-the-art models can serve as a scaffold for integrating multi-omics data, thereby enabling the identification of signatures of dysregulated metabolism by systems approaches. For example, increased plasma mannose levels due to decreased uptake in the liver have been identified as a potential biomarker of early insulin resistance by multi-omics approaches. In addition, we also review the emerging axis of human physiology and the human microbiome, discussing its contribution to host metabolism and quantitative approaches to study its variations in individuals.
-
Citations
Citations to this article as recorded by- Innovative Therapeutic Approaches in Non-Alcoholic Fatty Liver Disease: When Knowing Your Patient Is Key
Marta Alonso-Peña, Maria Del Barrio, Ana Peleteiro-Vigil, Carolina Jimenez-Gonzalez, Alvaro Santos-Laso, Maria Teresa Arias-Loste, Paula Iruzubieta, Javier Crespo
International Journal of Molecular Sciences.2023; 24(13): 10718. CrossRef - Oxymatrine Alleviates High-Fat-High-Fructose-Induced Fatty Liver in Rats: Understanding the Molecular Mechanism Through an Untargeted Metabonomics Study
Huan Li, Chang Wang, Qing Wang, Xuehua Liu, Juanjuan Zhang, He Zhang, Wenjie Fei, Hang Zhao, Luping Ren
Diabetes, Metabolic Syndrome and Obesity.2023; Volume 16: 4013. CrossRef - Research progress on inosine monophosphate deposition mechanism in chicken muscle
Zengwen Huang, Juan Zhang, Yaling Gu, Zhengyun Cai, Xiaofang Feng, Chaoyun Yang, Guosheng Xin
Critical Reviews in Food Science and Nutrition.2022; 62(4): 1062. CrossRef - Advances in Microbiome-Derived Solutions and Methodologies Are Founding a New Era in Skin Health and Care
Audrey Gueniche, Olivier Perin, Amina Bouslimani, Leslie Landemaine, Namita Misra, Sylvie Cupferman, Luc Aguilar, Cécile Clavaud, Tarun Chopra, Ahmad Khodr
Pathogens.2022; 11(2): 121. CrossRef - Multi-omics research strategies in ischemic stroke: A multidimensional perspective
Wentao Li, Chongyu Shao, Huifen Zhou, Haixia Du, Haiyang Chen, Haitong Wan, Yu He
Ageing Research Reviews.2022; 81: 101730. CrossRef - Combating Childhood Infections in LMICs: evaluating the contribution of Big Data Big data, biomarkers and proteomics: informing childhood diarrhoeal disease management in Low- and Middle-Income Countries
Karen H. Keddy, Senjuti Saha, Iruka N. Okeke, John Bosco Kalule, Farah Naz Qamar, Samuel Kariuki
EBioMedicine.2021; 73: 103668. CrossRef
- Innovative Therapeutic Approaches in Non-Alcoholic Fatty Liver Disease: When Knowing Your Patient Is Key
Letter
- Diabetes
- Letter: Trends in Hyperglycemic Crisis Hospitalizations and in- and out-of-Hospital Mortality in the Last Decade Based on Korean National Health Insurance Claims Data (Endocrinol Metab 2019;34:275–81, Ji Hong You et al.)
- Jang Won Son
- Endocrinol Metab. 2019;34(4):422-423. Published online December 23, 2019
- DOI: https://doi.org/10.3803/EnM.2019.34.4.422
- 3,521 View
- 40 Download
- 1 Web of Science
- 1 Crossref
-
PDFPubReader ePub
-
Citations
Citations to this article as recorded by- Incidence and predictors of hyperglycemic emergencies among adult diabetic patients in Bahir Dar city public hospitals, Northwest Ethiopia, 2021: A multicenter retrospective follow-up study
Melsew Dagne Abate, Ayele Semachew, Solomon Emishaw, Fentahun Meseret, Molla Azmeraw, Dawit Algaw, Dessie Temesgen, Sefineh Fenta Feleke, Ahmed Nuru, Makda Abate, Berihun Bantie, Atsedemariam Andualem
Frontiers in Public Health.2023;[Epub] CrossRef
- Incidence and predictors of hyperglycemic emergencies among adult diabetic patients in Bahir Dar city public hospitals, Northwest Ethiopia, 2021: A multicenter retrospective follow-up study
Editorial
- Exercise and Depression
- Jang Won Son
- Endocrinol Metab. 2015;30(3):270-271. Published online September 22, 2015
- DOI: https://doi.org/10.3803/EnM.2015.30.3.270
- 3,368 View
- 67 Download
Case Reports
- Obesity and Metabolism
- Two Cases of Allergy to Insulin in Gestational Diabetes
- Gi Jun Kim, Shin Bum Kim, Seong Il Jo, Jin Kyeong Shin, Hee Sun Kwon, Heekyung Jeong, Jang Won Son, Seong Su Lee, Sung Rae Kim, Byung Kee Kim, Soon Jib Yoo
- Endocrinol Metab. 2015;30(3):402-407. Published online May 18, 2015
- DOI: https://doi.org/10.3803/EnM.2015.30.3.402
- 4,880 View
- 60 Download
- 3 Web of Science
- 2 Crossref
-
Abstract
PDFPubReader
Allergic reaction to insulin is uncommon since the introduction of human recombinant insulin preparations and is more rare in pregnant than non-pregnant females due to altered immune reaction during pregnancy. Herein, we report two cases of allergic reaction to insulin in gestational diabetes that were successfully managed. One case was a 33-year-old female using isophane-neutral protamine Hagedorn human insulin and insulin lispro. She experienced dyspnea, cough, urticaria and itching sensation at the sites of insulin injection immediately after insulin administration. We discontinued insulin therapy and started oral hypoglycemic agents with metformin and glibenclamide. The other case was a 32-year-old female using insulin lispro and insulin detemer. She experienced pruritus and burning sensation and multiple nodules at the sites of insulin injection. We changed the insulin from insulin lispro to insulin aspart. Assessments including immunoglobulin E (IgE), IgG, eosinophil, insulin antibody level and skin biopsy were performed. In the two cases, the symptoms were resolved after changing the insulin to oral agents or other insulin preparations. We report two cases of allergic reaction to human insulin in gestational diabetes due to its rarity.
-
Citations
Citations to this article as recorded by- Non-glycemic Adverse Effects of Insulin
Alissa M. Guarneri , Robert P. Hoffman
Current Diabetes Reviews.2022;[Epub] CrossRef - Faulty Injection Technique: A Preventable But Often Overlooked Factor in Insulin Allergy
Partha Pratim Chakraborty, Sugata Narayan Biswas, Shinjan Patra
Diabetes Therapy.2016; 7(1): 163. CrossRef
- Non-glycemic Adverse Effects of Insulin
- Obesity and Metabolism
- Olanzapine-Induced Diabetic Ketoacidosis and Neuroleptic Malignant Syndrome with Rhabdomyolysis: A Case Report
- Young Kyoung Sa, Hyeon Yang, Hee Kyoung Jung, Jang Won Son, Seong Su Lee, Seong Rae Kim, Bong Yeon Cha, Ho Young Son, Chi-Un Pae, Soon Jib Yoo
- Endocrinol Metab. 2013;28(1):70-75. Published online March 25, 2013
- DOI: https://doi.org/10.3803/EnM.2013.28.1.70
- 3,953 View
- 37 Download
- 7 Crossref
-
Abstract
PDFPubReader
Atypical antipsychotics have replaced conventional antipsychotics in the treatment of schizophrenia because they have less of a propensity to cause undesirable neurologic adverse events including extrapyramidal symptoms, tardive dyskinesia, and neuroleptic malignant syndrome (NMS). However, atypical antipsychotics have been known to result in various metabolic complications such as impaired glucose tolerance, diabetes and even diabetic ketoacidosis (DKA). In addition, a number of NMS cases have been reported in patients treated with atypical antipsychotics, although the absolute incidence of neurologic side effects is currently significantly low. Here, we report a patient who simultaneously developed DKA, acute renal failure and NMS with rhabdomyolysis after olanzapine treatment. Olanzapine-induced metabolic complications and NMS were dramatically improved with cessation of the olanzapine treatment and initiation of supportive management including fluid therapy, hemodialysis, and intensive glycemic control using insulin. At short-term follow-up, insulin secretion was markedly recovered as evidenced by a restoration of serum C-peptide level, and the patient no longer required any hypoglycemic medications. Despite the dramatic increase in the use of atypical antipsychotics treatment, individualized treatments along with careful monitoring may be prudent for high risk or vulnerable patients in order to avoid the development of metabolic side effects.
-
Citations
Citations to this article as recorded by- Neuroleptic malignant syndrome in a patient with moderate intellectual disability treated with olanzapine: A case report
Francesco Piacenza, Suet Kee Ong, Patrick O’Brien, Maurice Clancy
Clinical Case Reports.2021; 9(4): 2404. CrossRef - Succinylcholine-Induced Rhabdomyolysis in Adults: Case Report and Review of the Literature
Robert William Barrons, Liem T. Nguyen
Journal of Pharmacy Practice.2020; 33(1): 102. CrossRef - Improvement in renal prognosis with prompt hemodialysis in hyperosmolar hyperglycemic state-related rhabdomyolysis
I-Wen Chen, Cheng-Wei Lin
Medicine.2018; 97(50): e13647. CrossRef - Treatment of Diabetic Ketoacidosis Associated With Antipsychotic Medication
Antonia Vuk, Maja Baretic, Martina Matovinovic Osvatic, Igor Filipcic, Nikolina Jovanovic, Martina Rojnic Kuzman
Journal of Clinical Psychopharmacology.2017; 37(5): 584. CrossRef - A Case of Primary Hypoparathyroidism Presenting with Acute Kidney Injury Secondary to Rhabdomyolysis
Abdullah Sumnu, Zeki Aydin, Meltem Gursu, Sami Uzun, Serhat Karadag, Egemen Cebeci, Savas Ozturk, Rumeyza Kazancioglu
Case Reports in Nephrology.2016; 2016: 1. CrossRef - Nanoneurotherapeutics approach intended for direct nose to brain delivery
Shadab Md, Gulam Mustafa, Sanjula Baboota, Javed Ali
Drug Development and Industrial Pharmacy.2015; 41(12): 1922. CrossRef - Brief Review of Articles in 'Endocrinology and Metabolism' in 2013
Won-Young Lee
Endocrinology and Metabolism.2014; 29(3): 251. CrossRef
- Neuroleptic malignant syndrome in a patient with moderate intellectual disability treated with olanzapine: A case report
 First
First Prev
Prev


